

Abstract
Introduction
Patients with sickle cell disease (SCD) suffer from frequent vaso-occlusive crises (VOC), the leading cause of hospitalization and emergency department (ED) visits for these patients. Patients and healthcare providers often report dissatisfaction with the quality of SCD pain management in the ED. Satisfaction has been defined as whether a patient's expectations about a health encounter were met. Infusion centers (IC) are alternatives to ED care for patients with VOC. The aim of this study is to describe adult patients' satisfaction with care for the treatment of uncomplicated VOC in EDs and ICs.
Methods
As part of a prospective cohort study (the ESCAPED study) comparing outcomes between ED and IC care for uncomplicated VOC, we conducted a descriptive analysis of patient satisfaction from the first acute visit of adult patients (>18 years) who were recruited from 4 sites (Baltimore, Baton Rouge, Cleveland, Milwaukee) from April 2015 to December 2016. Demographic and clinical variables were collected via medical record review. Participants were provided with a survey about their satisfaction of care within 72 hours after their acute visit to the ED or IC. The survey tool included questions about overall satisfaction with quality of care and with pain treatment received, satisfaction with pain management, communication with clinicians including physicians and nurses, interpersonal aspects of care, clinician competence, involvement of family and friends, and access to care. Responses were scored on a 7-point Likert scale from very strongly agree to very strongly disagree, except for "access to care" items, which were binary and categorical. We dichotomized Likert scale responses by grouping positive responses (very strongly agree, strongly agree, and agree) as being satisfied, and negative responses (very strongly disagree, strongly disagree, disagree, and uncertain) as being dissatisfied. Descriptive statistics were computed using Mann-Whitney U test for continuous variables and chi-squared test for categorical variables. All hypothesis testings were 2-sided and p values were not adjusted for multiple comparisons.
Results
We enrolled 483 patients in ESCAPED and followed them for 18 months. We excluded 115 patients who did not have VOC visits during their observation period. Of the 368 patients with visits, 212 patients (58%) responded to the survey after their first acute visit: 89 (42%) had received care at an ED and 123 (58%) received care at an IC. Patients who received care at an IC were older, more likely to be married or with a significant other, and less likely to live alone. More patients who had a history of kidney disease received care at an IC than in an ED. Patients with higher numbers of ED visits in the previous year were more likely to seek care in an ED and those with higher numbers of IC visits in the previous year were more likely to seek care at an IC.
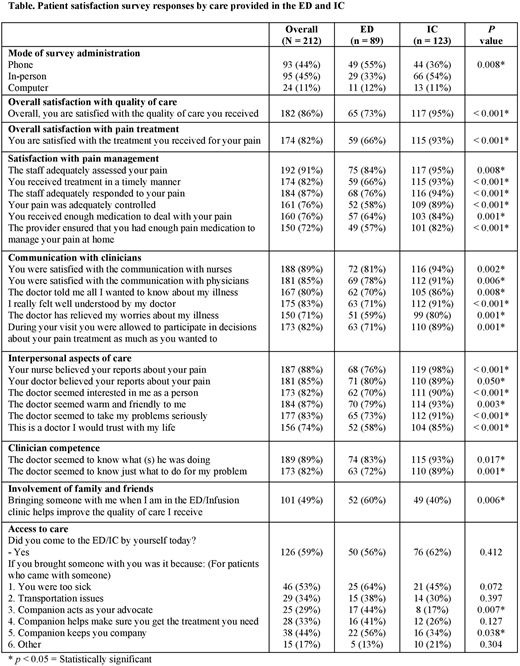
The majority of patients (55%) in the ED responded to the survey by phone whereas the majority of patients (54%) in the IC responded to the survey in-person. Overall, patients who received care in an IC were more satisfied with the quality of care (95% vs. 73%, p< 0.001) and with their pain treatment (93% vs. 66%, p< 0.001) than patients who received care in an ED. (Table) Adults who received care at an IC were more satisfied with the pain management, communication with clinicians, interpersonal aspects of care, and clinician competence than adults who received care at an ED. The majority of patients in both groups (59%) came for care unaccompanied; ED-treated patients were more likely than IC-treated patients to agree that a companion helped improve the quality of care they received.
Conclusions
Patients who received care in an IC were more satisfied with their care and with the quality of their pain management than patients who received care from an ED. Increasing access to IC models of care can improve delivery of patient-centered care for VOC.
Brooks:PCORI: Research Funding. Wang:PCORI: Research Funding. Seufert:PCORI: Research Funding. Haywood:PCORI: Research Funding. Varadhan:PCORI: Research Funding. Saheed:PCORI: Research Funding. Segal:PCORI: Research Funding. Field:Incyte: Research Funding; Ironwood: Consultancy, Research Funding; Prolong: Research Funding. Frymark:PCORI: Research Funding. Little:Doris Duke Charitable Foundations: Research Funding; NHLBI: Research Funding; Hemex: Patents & Royalties: Patent, no honoraria; PCORI: Research Funding. Griffin:PCORI: Research Funding. Arnold:PCORI: Research Funding. Shows:PCORI: Research Funding. Piehet:PCORI: Research Funding. Proudford:PCORI: Research Funding. Robertson:PCORI: Research Funding. Wallace:PCORI: Research Funding. Kincaid:PCORI: Research Funding. Green:PCORI: Research Funding. Burgess:PCORI: Research Funding. Lanzkron:Selexys: Research Funding; Pfizer: Consultancy, Research Funding; GBT: Consultancy, Research Funding; Prolong: Research Funding; NHLBI: Research Funding; PCORI: Research Funding; Ironwood: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal